Auditory Integration Training
“My 10-year-old child stated after a couple of days into the AIT therapy: ‘The buzzing sound is gone!’. His reading and writing has improved. There has been a great decrease in anxiety.”
The neurodevelopmental approach is based on neuroplasticity: the central nervous system can be “rewired” providing the proper stimulation. It addresses the behavioral and learning inefficiencies of an individual looking at the steps of brain development from the lower level (the foundation) to the highest centres (the roof). It considers which functions of the central nervous system (CNS) should be in place from birth to seven-years old (grade two) in order to be an efficient learner able to use his attention span and self-regulate his behavior. This approach looks at the “input” of information coming from the visual, auditory, and tactile domains in order to yield the necessary quality “output” in the manual, language, and mobility areas.
The primary reflexes should be in place in the human body from conception. The reflexes emerge at different periods of the brain development. As they are integrated they give rise to more mature neurological functions. When these reflexes are not integrated, they yield inefficiencies in motor control, eye-hand coordination, sensory perception, emotional behaviour, attention, and/or higher cognitive abilities.
The term ‘stimulus-response arc’, or what is more commonly referred to as a reflex can be described as being a stereotyped response of the CNS to a specific stimulus of an individual. The nervous system’s organization is hierarchical moving from the lowest levels lodged in the spinal cord and brain stem, through the midbrain wincluding the limbic system, toward the highest levels which are the cortex for processing and the pre-cortex to manage self-control. This neurological organization develops through movement patterns in stages from conception to the toddler. These reflexes are called primitive reflexes. The primitive reflexes present from conception are organized in a hierarchy. These reflexes allow the baby to make body movements. When these movements are done in the right proportion and the proper sequence, they contribute to inhibit these primitive reflexes and give place to higher neurological organizations called ‘functions’. The higher functions of the CNS relate to learning (memory, ability to categorize, logic) and to attention span (arousal and inhibition). Let me give you an analogy. Lets pretend that the brain is a building with a phone relay in its center (thalamus). Over the years, the electric connections are used then replaced by newer ones. However, if certain connections are not removed because they have not been used enough, the actual phone relay may still have connections from 1950 which makes the whole system inefficient. When the primitive reflexes are not integrated we find their manifestations in children who struggle with different forms of learning. Sally Goddard from the Institute of Neuro-physiological Psychology has done an amazing work in this area of primary reflexes. Let us look at the most commonly active reflexes found in children with learning and attention inefficiencies.


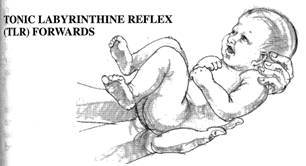
Note: The four pictures on this page illustrate some of the favorite positions characteristic of people (children, teens and even adults) when these reflexes are not integrated. This lack of integration keeps the person from reaching the maturity of postural reflexes that is a step further in the integration of higher levels of organization of the central nervous system.
The term “stimulus-response arc,” or what is more commonly referred to as a “reflex,” can be described as being an automatic response of the CNS to a specific stimulus. The central nervous system is the only hierarchical system of the body. The nervous influx enters the brainstem from the spinal cord (via the reticular formation), to the midbrain (including the limbic system), to the cortex which is responsible for sensori-motor processing and association. The pre-cortex is the final step in that hierarchy and manages planning and self-control.
This neurological organization develops in stages, hierarchy, through movement patterns from conception to the toddler years. These reflexes are called primary reflexes. These reflexes allow the baby to make body movements. When these movements are done in the right proportion and the proper sequence, they contribute to integrating these primitive reflexes and give place to higher neurological organization called “functions.” The higher functions of the CNS relate to learning (memory, ability to categorize, logic), to attention span (arousal and inhibition) leading ideally to self-regulated behaviour.
Here is an analogy to help you understand. Let’s pretend that the brain is a building with a phone relay in its center (thalamus). Over the years, the electric connections are used, then replaced by newer ones. However, if certain connections are not removed because they have not been used enough, the phone relay will have connections from 1950 that make the whole system inefficient. When the primary reflexes are not integrated, we find their manifestations in children who struggle with different forms of learning, attention span, and behaviour dis-regulation.
“Non-integrated primitive movement patterns or reflexes force a person to function on a survival level. Survival leads to a narrowing of the attention span, lack of “cause and effect” in thinking, and poor spontaneous control of movements, skills and behaviour. As a result of this limited experience, a person automatically chooses “freezing” or “fight and flight” defense strategies for organizing his thinking and behaviour. The “choice” at a higher reasoning level is not available for this person, and they demonstrate lower motivation for learning and achievement.” – Svetlana Masgutova, Russian psychologist, Integration of Infant Dynamic and Postural Reflex Patterns
Sally Goddard from the Institute of Neuro-Physiological Psychology has done amazing work in the area of primary reflexes. Let us look at five reflexes that are most commonly found “non-integrated” in people with different cognitive and emotional issues.
The Fear Paralysis Reflex is a withdrawal reflex that emerges in the embryonic stage. During this .stage the embryo reacts to stress and stimulation by withdrawing and freezing. As the foetus’ tactile awareness develops, withdrawal upon contact gradually lessens. It is thought that this reflex is the first step in learning to cope with stress. Ideally, the FPR merges into the Moro reflex and has become inactive before birth. If the FPR is not fully integrated at birth it may contribute to life-long challenges related to fear. People with the FPR active may often be very anxious and tend to veer towards negativity which can prevent them from easily moving forward to living a meaningful, interactive life. An active FPR often goes hand-in-hand with an un-integrated Moro reflex.

The Moro reflex, one of the most basic and important reflexes to influence emotion and learning, emerges at nine weeks in utero and
is fully present at birth. It should be integrated by four months after birth. The integrated Moro reflex should give place to the Strauss reflex (startle reflex). The Moro reflex manifests itself in a sudden movement of the arms extending with opening of the fingers and with legs folded, with a momentary freeze before the coming back of the arms and legs in a closed position.
The tonic labyrinthine reflex (TLR) emerges in utero, is present at birth, and integrated at approximately four months after birth. As the head moves away from the spine, the arms and the legs extend (when the head moves backward) and they will curl when the head moves forward.
(Ex: the impact is observed in a gravity-free environment as astronauts start “mirror-writing”)


The asymmetrical tonic neck reflex (ATNR) emerges at 18 weeks in utero, is present at birth, and should be integrated at six months. When the baby’s head moves to one side, the arm and leg of the same side extend while the limbs of the other side bend. Most published research and articles on primary reflexes point to this reflex as being the most actively involved in the learning and attention span functions. This is called the “learning reflex.”
The symmetrical tonic neck reflex (STNR) emerges at six-to-nine months of life and should be integrated by 11 months. It manifests itself in the “creeping” movement of the baby on his hands and knees.
It may be seen as a stage of the labyrinthe reflex because of the crucial involvement of the vestibular system. Bender (1976) estimated that 75% of learning disabled children have retained STNR.

TLR: front and back
ATNR: right and left
STNR: from the waist up and from the waist down
Other important primary reflexes are addressed in our work: the Spinal Galant Reflex, the Grasp or Palmar Reflex, the Sucking Reflex, the Babinski Reflex.
This article is summarizing some of the reflexes that, when not integrated in a person, are part of the neurological root-based causes of labels such as Learning Disability, Dyslexia, Dysgraphia, Attention Deficit Disorder, Autism, Depression, Anxiety and many others. It is possible to give a second chance to the brain in providing the right movement patterns in the proper sequence: that is what neurodevelopmental functional re-organization is all about
Suzanne Day, Neuropsychologist (Québec)
Blomberg, Harald (2011) Movements That Heal
Goddard, Sally (2002) Reflexes, Learning, and Behavior
Goddard, Sally (2008) What Babies and Children Really Need
Goddard, Sally (2009) Attention, Balance and Coordination
Goddard, Sally (2004) The Well Balanced Child
Masgutova, Svetlana (2002) Integration of Infant Dynamic and Postural Reflex Patterns
Pheloung, Barbara (2004) Help your Child to Learn
Teitelbaum, Osnat and Philip (2008) Does Your Baby Have Autism?