Auditory Integration Training
“My 10-year-old child stated after a couple of days into the AIT therapy: ‘The buzzing sound is gone!’. His reading and writing has improved. There has been a great decrease in anxiety.”
Pertinent and effective intervention can be planned only when some of the causes are identified. As a neuropsychologist, I have found that the best way to efficiently increase the learning, behavior and emotional self-regulation is to look at the root cause of the problem in terms of the development of brain functions. This neurodevelopmental approach based on sequential and rhythmic movements has proven to be invaluable. This approach looks at the condition of the functions that should be in place from birth to seven-years old in the areas of visual, auditory, tactility, mobility, manual, and language.
When addressing the learning and behavioral issues, the inefficient functions of the central nervous system must be addressed. The central nervous system (CNS) is comprised of the spinal cord and the brain. The different parts of the CNS communicate with electrical impulses, which are transmitted along the nerve cells and generated by chemical markers called neurotransmitters.
Dr. Yancopoulus and his team have identified protein-like markers, which guide the dendrites (the extremities of nerve cells) to their specific destinations “…during development, nerve cells talk to muscles cells by sending a chemical code in the form of the neurotransmitter acetylcholine.” Acetylcholine originates in the brainstem which is the first step of the hierarchy of brain development. Acetylcholine is involved in the development of the working memory and attention span, the ability to stay on task (vigilance), the sensory processing, as well as the capacity of neuroplasticity to create new pathways.
When discussing learning and behavioural issues we mainly refer to the cortex (of the brain). However, the central nervous system (CNS) is a hierarchical system, with important pathways bringing the nervous influx from our senses to the spinal cord, the brainstem and through the reticular formation to the midbrain, the cortex, and finally to the pre-cortex. The brainstem (the medulla and the pons) is a crucial section of the CNS that is often neglected when talking about learning and behavioural issues; it is located between the spinal cord and the midbrain.
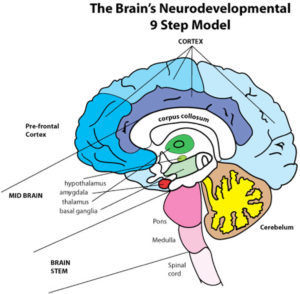
Rhythmic movements originate in the brainstem. It regulates both motor and sensory processes, consciousness, and the control of perception. The brainstem constitutes bulges of nerve pathways carrying the nerve impulses between the brain and the body. The brainstem houses not only the reticular formation (network of nerves) responsible for vigilance (alertness), but also the nuclei where the main neurotransmitters originate. It is very interesting to note, also, that the twelve pairs of cranial nerves originate in the brainstem. Some of them are motor nerves, like the oculomotor nerves, which pertain to the eyes. Some are sensory, like the olfactory nerve, and some have mixed functions like the trigeminal nerve.
All sensory Information is transferred from the brainstem to the thalamus located in the midbrain. The thalamus is like a telephone switchboard that in turn directs information to different areas of the cortex, except for smell, which goes directly to the cortex bypassing the “switchboard”.
What happens in the cortex is the result of loops along the central nervous system pathway from the brainstem to the cortex. We know for example, that reading happens mainly in the left temporal lobe of the cortex, while the quality of one’s attention span depends upon the pre-frontal cortex.
The pre-frontal cortex is responsible for higher executive functions like planning, flexibility, and decision-making. Any information from the brainstem that is missed along the way creates processing inefficiencies. For example, if the child has not crawled enough, or not at all, the child’s body image of himself in space will be incomplete. Indeed, when the child is on his tummy to crawl, the sensory information coming from the dermatomes located on his skin “… feed into the sensory thalamus … the impulses received from the nerve endings create a kind of holographic image of his body in the thalamus.” (Svea Gold). The thalamus is the brain generator of electricity or switchboard for the nervous impulses. When the child crawls and creeps,the cortex and pre-crotex (last steps of the hierarchy of the brain development) get the correctsensory information from the switchboard. The quality of this sensory informationstored in the thalamus will allow the cortex and pre-cortex to use it in abstract reasoning using and understandingspatial terms such as “long and short,”“forward,” “extended,” “oversized.” etc.
Dr. Temple Fay, Glen Doman and Carl Delacato, who started their work in the fifties, are giants in this field of neuroplasticity interventions aiming to improve learning processing and attention span. These clinicians clearly showed that an interruption of the natural development of the central nervous system (CNS) in a child brings about incomplete brain organization.This prohibits the child from achieving his maximum potential. Working mainly, at first, with brain-injured children, they observed that these children could not make the stereotype movements that a normal child could. By helping brain-injured children make these movements, they also discovered that the children would start doing these movements by themselves. Calling this intervention Neurological Reorganization, they framed their discovery in a developmental profile. Dr. Temple Fay’s Profile of Development (click for profile) This developmental profile explains clearly the sequential development of the CNS from birth to seven-years old, and the simultaneous development of different areas such as vision, auditory, tactility, language, mobility, and manual functions. Following this pattern of sequential development should bring about complete brain organization, and then in turn the child would attain his maximum potential. Unfortunately, children with learning disabilities cannot access their full potential because of the inefficiencies in the neurodevelopment of their CNS.
By observing how a child’s brain receives, processesand retrieves information through his senses, specific inefficiencies are identified. – Input/Output list of symptoms (click here)
The neurodevelopment approach considers how the skin and the muscles, the ears and the eyes are transporting information to the brain. For example, eye convergence is often a problem with people who have learning, attention and/or behavioural difficulties. Convergence is the ability of the eyes to work synchronously (together). When the eyes do not converge, a degree of double vision is experienced which confuses the person, who will then “squint” in his attempt to eliminate his double vision. Subsequently, reading and writing are difficult. Eye exercises can correct this problem. However, it is only when we understand the connections between the eyes and the brainstem that we can intervene more efficiently. Masao Ito from the University of Tokyo explains how the loops between the functions of the semi-circular canals in the inner ear, the cerebellum, and the eyes not only affect posture and balance (for example being seasick) but also affects hearing and speech.
“Vestibular and neck reflexes stabilize the head and eyes… Both reflexes produce coordinated effects on the muscles of the arms, legs and neck. Movements of the head also evoke vestibular-ocular reflexes that stabilize visual images on the retina.” Eric Kandell, Principles of Neural Science
Another problem with learning challenges, emotional (such as depression and anxiety), and behavioural issues (such as attention deficit), is the difficulty a person has when doing multi-tasks (more than one thing). Often these children have not developed an efficient cross pattern movement and are lacking the speed needed in their processing. The speed of processing is generated by the production of myelin on the nerve cells. The myelin grows as the nerve influx passes through the same pathways. The largest fiber bundle in the brain,also the richest in myelin, is the corpus callosum that connects the two hemispheres of the brain. People who have learning difficulties lack development in the corpus callosum. Developmental exercises like crawling and creeping can be used to stimulate these functions. Understanding how the child’s brain receives the information allows us, in subsequent steps, to concentrate on how the person processes the information, stores and utilizes it.
Research states that up to 70% of children with attention problemsoften have learning disabilities. Attention problems present a wide range of symptoms. One of the frequent symptoms is sensory dysfunction or lack of efficiency in dealing with sensory information. Each of the senses has a specific function in the learning process that channels the information to the brain. When facing behaviour problems such as impulsivity, hyperactivity, aggressiveness, and reduced attention span, investigating the sensory system broadens our perspective and increases our efficiency in treating the symptoms as we recognize the root causes.
The sensory system can have one of two types of sensory dysfunctions: “hyper” which leads to an over-sensitive reaction to information, and the “hypo,” which yields an under-sensitive state.
“Where there is arousal, internal excitation and muscle tension increase. Where there is prolonged muscle tension eventually there is fatigue. Fatigue will reduce performance, so that in order to maintain the same level of performance and make up for the lack of efficiency, there will need to be an increased level of arousal. Thus a vicious circle is created.” Sally Goddard from the Institute for Neuro-Physiological Psychology in England
Many children, and adults, presenting tactile issues ask to have the tags from the back of their clothes removed; they are hyper-sensitive to surface touch. However, these people are “very tough” to pain when at the dentist, or children would complain of ear infections only when the eardrum bursts: they are hypo-sensitive to deeper touch. People who constantly need to support their body or be barely able to keep still, usually are hypo-sensitive to deeper touch. They often need to feel pressure and consequently will move, lean on or over things, and can be aggressive toward other children. The surface and the deep touch sensation are processed in two different parts of the brain: when one is “on” the other is “off.” The good news is that something can be done to balance the brain’s perceptual dis-regulation.
Another example is the child who is sensitive to sunlight and fluorescent lighting; s/he would be considered hyper-visual. A delay in the closing of the retina keeps this child in a state of inner “alert” in relation to light. The hypo-sensory visual child will have difficulty in keeping order in his room even though his mind would be able to perceive complex three-dimensional designs.
Also, children who are hyper-sensitive to noises will be easily distracted in a large group or to any sharp sound. Hyper-auditory children have difficulty concentrating because they do not adequately filter noises. They will often disconnect from the environment if they are forced to stay in a situation with auditory overload. A better understanding of these individual limitations help parents and educators to be more patient in disciplining this type of child instead of punishing him for not meeting certain behavioural standards. The child needs help in developing a more balanced perception in order to meet social demands with less energy.
When the brain seems to misinterpret the information brought in from the senses and the muscles, the objective of treatment is to normalize the brain’s perception of the information coming from the sensory input through the afferent pathways, and the motor output through the efferent pathways. The treatment, through specific, targeted repetition of sequential rhythmic movements, aims the stimulation at the functions of the central nervous system (CNS) responsible for efficient processes. Svea Gold, who first witnessed amazing changes in her child, had spent thirty years trying to understand through the exponential brain research how this change was possible. She summarized beautifully:
“It (the program of activities) makes children go through the same movements which the early reflexes would have dictated their little bodies to make, these same movements will create chemicals at the junction of the muscle and the axons and the chemical markers will make sure that the messages go to the exact part of the brain that nature intended them to go… we allow the brain to repair itself.” If Kids Just Came with Instruction Sheet, by Svea Gold
Indeed, we are wonderfully designed.
I have used this approach for the past twenty years. One of the tests being used to measure a child’s progress is the ‘Draw a Person’ test: the child is asked to draw a picture of himself. The drawing reflects how he perceives himself in space.
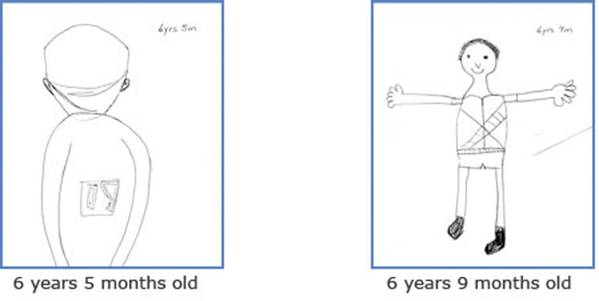
Notice after just 4 months on the program, the addition of the arms, hands and ears, which suggests that he has grown in his perception of these body parts. The mother commented how talkative he was now and how willing he was to sit still and put effort into his reading. Three months later, more significant changes were observed: the arms are now down which gives a more mature awareness of himself in space; the head proportion is closer to reality.
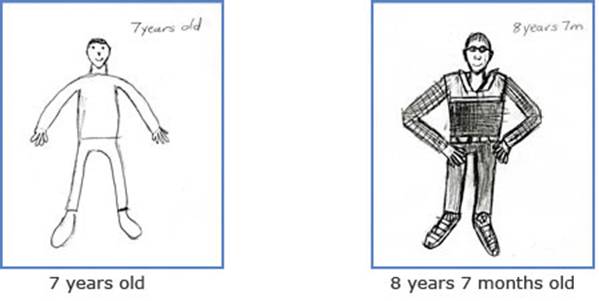
The mother reports that he has stopped hiding under the covers and can walk in a darkened area. Drooling and feet dragging have virtually disappeared.One year later, the level of maturity is beyond what we would expect from a 8-year old child.The mother reports a continual marked improvement in his speech. Then, two years after the first visit, the mother concludes that his disfluent speech is not apparent anymore as well as he is more confident and outgoing and less fearful.
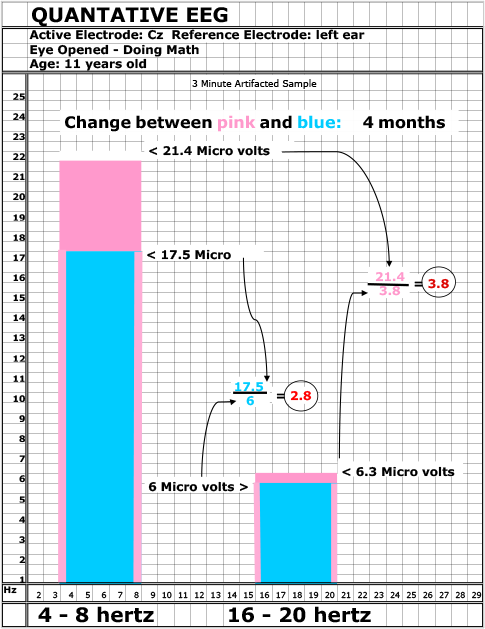
Quantitative EEG (QEGG) measurements were used to witness the changes in brain wave patterns of children who have been doing a neurodevelopmental program for only a few months. Learning and attention difficulties are characterized by a larger production of theta waves, the slow waves responsible for the “tune out”mind set. The faster beta waves are responsible for the “problem solving” mind set. After a few months of doing neurodevelopment activities, the QEGG measurement usually shows a reduction in the production of theta waves, leading to a more balanced and normal ratio between the theta (slow) and the beta (faster) waves.
Below is an example shown on a bar graph. From right-to-left we have the frequency of the waves, the slower waves being at zero and the faster being twenty. The blue line shows the brain wave pattern of the child when he first came in with attention problems and difficulties with math. The ratio between the slow waves and the faster waves is 4.1. According to Lubar and Monastra’s research (1999), a ratio above 2.7 is significant of an attention problem. After a few months of doing the neurodevelopmental activities at home he showed a marked improvement in producing fewer theta waves, 4-8 hertz. The ratio between the slow waves (theta) and the faster waves (beta) was then 3.1. The post-test results are shown in the pink lines.
The mother described her child as being more attentive. This child presented with math dificulty although without problems understanding concepts. The mom reported that he was scoring only 60% average in spite of using a very good math curriculum and receiving math tutoring. After the neurodevelopment program of activities, the mother was delighted with 90% achievement on all his math tests. A remarkable change in just a four month period.
Suzanne Day, Neuropsychologist (Québec)